
Open Access
Cognitive Functional Therapy
Research
Cognitive Functional Therapy: An Integrated Behavioral Approach for the Targeted Management of Disabling Low Back Pain
Peter O'Sullivan, JP Caneiro, Mary O'Keefe, Anne Smith, Wim Dankaerts, Kjartan Fersum, Kieran O'SullivanPhysical Therapy & Rehabilitation Journal, Volume 98, Issue 5, 1 May 2018, Pages 408-423, https://doi.org/10.1093/ptj/pzy022
Summary
Section 1 - "Multidimensional Factors Associated with Disabling LBP"
Section 2 - "Cognitive Functional Therapy: Assessment and Treatment"
Section 3 - "Skills Required to Implement CFT"
From Fear to Safety: A Roadmap to Recovery From Musculoskeletal Pain
JP Caneiro, Anne Smith, Samantha Bunzli, & Steven J. Linton
Physical Therapy & Rehabilitation Journal, Volume 102, Issue 2, 23 December 2021, https://doi.org/10.1093/ptj/pzab271
Summary
Fear learning
Safety-learning
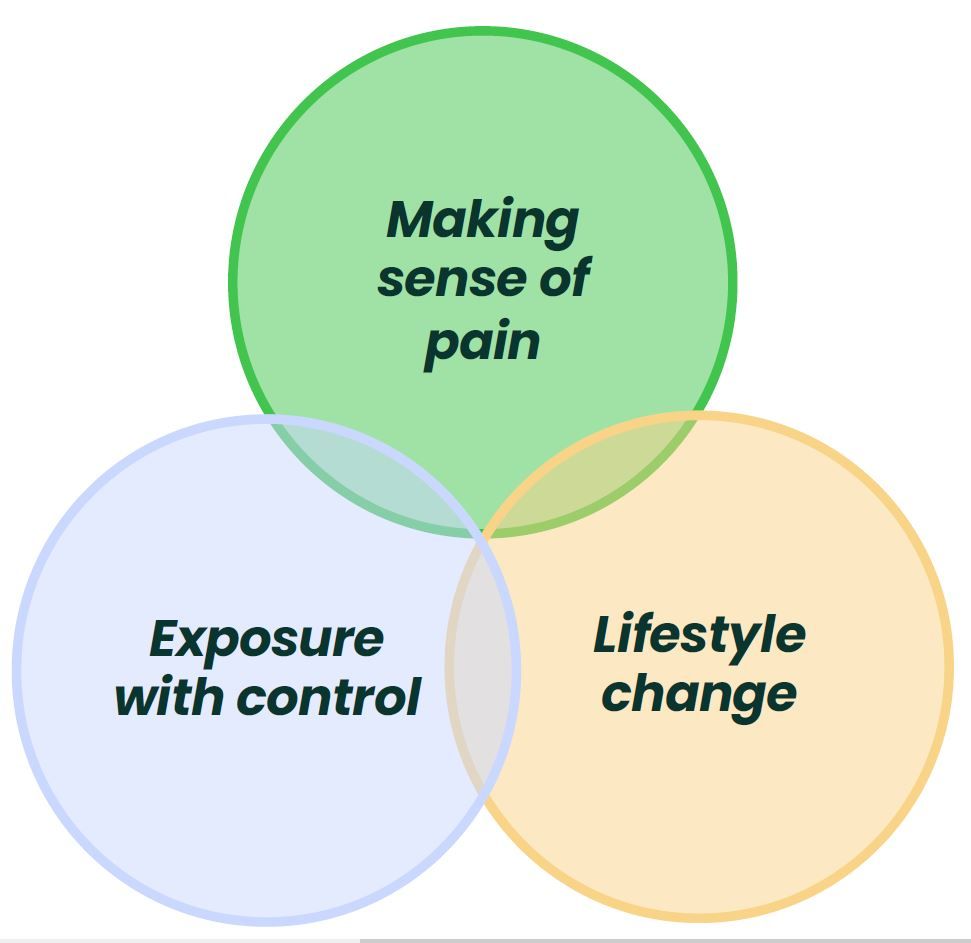
CFT to promote safety-learning
Patient-centered consultations for persons with musculoskeletal conditions
Joletta Belton, Hollie Birkinshaw & Tamar Pincus
Chiropractic & Manual Therapies, Volume 30, Issue 53, 2022, https://doi.org/10.1186/s12998-022-00466-w
Summary
Patient Perspectives on Participation in Cognitive Functional Therapy for Chronic Low Back Pain
Samantha Bunzli, Sarah McEvoy, Wim Dankaerts, Peter O'Sullivan, Kieran O'Sullivan
Physical Therapy, Volume 96, Issue 9, 1 September 2016, Pages 1397–1407, https://doi.org/10.2522/ptj.20140570
Summary
Methods
Two themes emerged from the interviews:
Theme 1 - Changing Pain Beliefs
Theme 2 - Achieving Independence
Physiotherapists report improved understanding of and attitude toward the cognitive, psychological and social dimensions of chronic low back pain after Cognitive Functional Therapy training: a qualitative study
Aoife Synnott, Mary O’Keeffe, Samantha Bunzli, Wim Dankaerts, Peter O'Sullivan, Katie Robinson, Kieran O'Sullivan.
Journal of Physiotherapy, Volume 62, Issue 4, October 2016, Pages 215-221, https://doi.org/10.1016/j.jphys.2016.08.002
Summary
Methods

Four themes emerged from the interviews:
Theme 1
Theme 2
Theme 3
Theme 4
Physiotherapists’ validating and invalidating communication before and after participating in brief Cognitive Functional Therapy training. Test of concept study
Riikka Holopainen, Mikko Lausmaa, Sara Edlund, Johan Carstens-Söderstrand, Jaro Karppinen, Peter O’Sullivan & Steven J. Linton
European Journal of Physiotherapy, Volume 25, Issue 2, 23 September 2021, Pages 73-79, https://doi.org/10.1080/21679169.2021.1967446
Riikka Holopainen, Mikko Lausmaa, Sara Edlund, Johan Carstens-Söderstrand, Jaro Karppinen, Peter O’Sullivan & Steven J. Linton
European Journal of Physiotherapy, Volume 25, Issue 2, 23 September 2021, Pages 73-79, https://doi.org/10.1080/21679169.2021.1967446
Summary
Methods
Results
Cognitive Functional Therapy with or without movement sensor biofeedback versus usual care for chronic, disabling low back pain (RESTORE): a randomised, controlled, three-arm, parallel group, phase 3, clinical trial
Peter Kent, Terry Haines, Peter O'Sullivan, Anne Smith, Amity Campbell, Robert Schutze, Stephanie Attwell, JP Caneiro, Robert Laird, Kieran O'Sullivan, Alison McGregor, Jan Hartvigsen, Den-Ching A Lee, Alistair Vickery, Mark Hancock. The Lancet, Volume 401, Issue 10391, 3 June 2023, Pages 1866-1877, https://doi.org/10.1016/S0140-6736(23)00441-5
Peter Kent, Terry Haines, Peter O'Sullivan, Anne Smith, Amity Campbell, Robert Schutze, Stephanie Attwell, JP Caneiro, Robert Laird, Kieran O'Sullivan, Alison McGregor, Jan Hartvigsen, Den-Ching A Lee, Alistair Vickery, Mark Hancock. The Lancet, Volume 401, Issue 10391, 3 June 2023, Pages 1866-1877, https://doi.org/10.1016/S0140-6736(23)00441-5
Summary
Methods
Results
What do the results mean?
It's time for a change with the management of non-specific chronic low back pain.
Peter O'Sullivan. British Journal of Sports Medicine, Volume 46, Issue 4, 1 March 2012, Pages 224-227, https://doi.org/10.1136/bjsm.2010.081638
Peter O'Sullivan. British Journal of Sports Medicine, Volume 46, Issue 4, 1 March 2012, Pages 224-227, https://doi.org/10.1136/bjsm.2010.081638
Summary

From protection to non-protection: A mixed methods study investigating movement, posture and recovery from disabling low back pain
Kevin Wernli, Anne Smith, Fiona Coll, Amity Campbell, Peter Kent, Peter O'Sullivan. British Journal of Sports Medicine, Volume 26, 12 August 2022, Pages 2097-2119, https://doi.org/10.1002/ejp.2022
Kevin Wernli, Anne Smith, Fiona Coll, Amity Campbell, Peter Kent, Peter O'Sullivan. British Journal of Sports Medicine, Volume 26, 12 August 2022, Pages 2097-2119, https://doi.org/10.1002/ejp.2022
Summary

A Prospective Qualitative Inquiry of Patient Experiences of Cognitive Functional Therapy for Chronic Low Back Pain During the RESTORE Trial
Nardia-Rose Klem, Peter O’Sullivan, Anne Smith, and Robert Schütze. Qualitative Health Research, 9 September 2024, https://doi.org/10.1177/10497323241268777
Nardia-Rose Klem, Peter O’Sullivan, Anne Smith, and Robert Schütze. Qualitative Health Research, 9 September 2024, https://doi.org/10.1177/10497323241268777
Summary
What Influences Patient-Therapist Interactions in Musculoskeletal Physical Therapy? Qualitative Systematic Review and Meta-Synthesis
Mary O'Keeffe, Paul Cullinane, John Hurley, Irene Leahy, Samantha Bunzli, Peter B. O'Sullivan, Kieran O'Sullivan. Physical Therapy, 1 May 2016, Volume 96, Issue 5, Pages 609-622, https://doi.org/10.2522/ptj.20150240
Mary O'Keeffe, Paul Cullinane, John Hurley, Irene Leahy, Samantha Bunzli, Peter B. O'Sullivan, Kieran O'Sullivan. Physical Therapy, 1 May 2016, Volume 96, Issue 5, Pages 609-622, https://doi.org/10.2522/ptj.20150240
Summary
Patients with worse disability respond best to cognitive functional therapy for chronic low back pain: a pre-planned secondary analysis of a randomised trial
Mark Hancock , Anne Smith , Peter O’Sullivan , Robert Schütze , JP Caneiro, Jan Hartvigsen, Kieran O’Sullivan, Alison McGregor, Terry Haines, Alistair Vickery, Amity Campbell, Peter Kent. Journal of Physiotherapy, 16 October 2024, Volume 70, Issue 4, Pages 294-301, https://doi.org/10.1016/j.jphys.2024.08.005
Mark Hancock , Anne Smith , Peter O’Sullivan , Robert Schütze , JP Caneiro, Jan Hartvigsen, Kieran O’Sullivan, Alison McGregor, Terry Haines, Alistair Vickery, Amity Campbell, Peter Kent. Journal of Physiotherapy, 16 October 2024, Volume 70, Issue 4, Pages 294-301, https://doi.org/10.1016/j.jphys.2024.08.005
Summary
The "future" pain clinician: Competencies needed to provide psychologically informed care
Steven J Linton, Peter B O'Sullivan, Hedvig E Zetterberg, Johan W S Vlaeyen. Scandinavian Journal of Pain, 8 August 2024, Volume 24, Issue 1, Pages 294-301, https://doi.org/10.1515/sjpain-2024-0017
Steven J Linton, Peter B O'Sullivan, Hedvig E Zetterberg, Johan W S Vlaeyen. Scandinavian Journal of Pain, 8 August 2024, Volume 24, Issue 1, Pages 294-301, https://doi.org/10.1515/sjpain-2024-0017
Summary
Mechanisms of change in cognitive functional therapy: A longitudinal mediation analysis of the RESTORE clinical trial for disabling chronic low back pain
Robert Schütze, Bernard Liew, JP Caneiro, Peter O’Sullivan, Peter Kent, Mark Hancock, Jan Hartvigsen, Kieran O’Sullivan, Alison McGregor, Amity Campbell, Stephanie Attwell, Anne Smith. Behaviour Research and Therapy, 3 September 2025, Volume 193, Article 104853, https://doi.org/10.1016/j.brat.2025.104853
Robert Schütze, Bernard Liew, JP Caneiro, Peter O’Sullivan, Peter Kent, Mark Hancock, Jan Hartvigsen, Kieran O’Sullivan, Alison McGregor, Amity Campbell, Stephanie Attwell, Anne Smith. Behaviour Research and Therapy, 3 September 2025, Volume 193, Article 104853, https://doi.org/10.1016/j.brat.2025.104853
Background
Study Design

Cognitive Functional Therapy:
An Integrated Behavioral Approach for the Targeted Management of Disabling Low Back Pain
Summary
Section 1 - "Multidimensional Factors Associated with Disabling LBP"
Section 2 - "Cognitive Functional Therapy: Assessment and Treatment"
Section 3 - "Skills Required to Implement CFT"
From Fear to Safety: A Roadmap to Recovery From Musculoskeletal Pain
Summary
Fear learning
A hybrid learning portal integrating cutting-edge research, clinical innovations,
and resources for the treatment of musculoskeletal pain.
© Copyright 2026
Evoolve Pain Care Academy Pty Ltd (ABN 13672998168)
215 Nicholson Rd, Shenton Park,
Western Australia 6008
